Summary
- Reloxaliase has a >80% probability of reaching commercial stage after reviewing the results of the URIROX-1 trial and the design of the URIROX-2 trial.
- Reloxaliase has a shot at $22 billion/year revenue opportunity just in the U.S. with a competitive advantage, yet the company's pipeline is being valued at just $45M.
- The stock is at a good Buy level after the recent pullback. Rating Buy, first price target=$4.50/share, time-frame=1-2 years.
- I do much more than just articles at Vasuda Healthcare Analytics: Members get access to model portfolios, regular updates, a chat room, and more. Get started today »
![]()
Allena Pharmaceuticals (ALNA) was founded in 2011 and is based in Newton, Massachusetts. The company's development pipeline is focused on the development, discovery, and commercialization of oral enzyme therapeutics to treat patients with kidney diseases. Its lead product candidate is Reloxaliase, an oral enzyme therapeutic for the treatment of enteric hyperoxaluria (EH) in adults. For the purpose of this article, I should focus on the EH pipeline of the company.
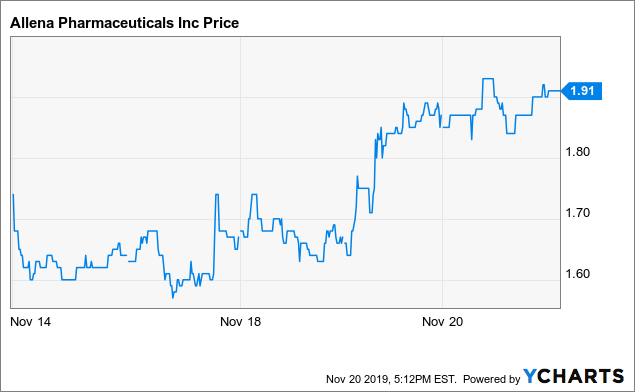 Data by YCharts
Data by YChartsScope of the problem:
Hyperoxaluria is characterized by high levels of oxalate in the plasma. In healthy individuals, up to half of the urinary oxalate is derived from the diet. Under normal conditions, all oxalate absorbed from the diet and produced endogenously is excreted in the urine. Normal urinary oxalate excretion is variable but urinary oxalate excretion greater than 40 to 45 mg per day is considered hyperoxaluria.
Primary hyperoxaluria is a genetic disease that results from certain genetic mutations and is classified into 3 different types. Enteric hyperoxaluria results due to certain disorders like gastric bypass surgery, inflammatory bowel disease, IBD (e.g. Crohn's disease), short-bowel syndrome, celiac disease, ileal resection, and chronic pancreatitis which lead to access absorption of oxalate in the G.I. tract. While systemic oxalate deposition in the heart, joints, bones and peripheral nerves is seen in primary hyperoxaluria, such manifestation is rare in secondary causes like EH. This may be due to lower systemic oxalate load in EH.
The pathophysiology of EH in IBD results due to an increase in oxalate solubility in the intestinal lumen and an increase in bowel permeability to oxalate due to bile salts and colonic mucosal inflammation. Normally, dietary calcium binds to dietary oxalate to form insoluble calcium oxalate, CaOx, that is excreted in the stool. In EH, non-absorbed fatty acids bind to calcium in the small intestine and thus dietary calcium is unable to bind to dietary oxalate. Dietary oxalate is present in high amounts in the intestinal lumen and is absorbed in the blood from the colon. in IBD, a lack of oxalate degrading bacteria in the colon (due to the disease state, change in diet or administered antibiotics) is also thought to result in an increase in intestinal oxalate absorption. The prevalence of CaOx stones after intestinal resection in Crohn's disease is estimated at 28%.
In intestinal malabsorption syndromes, a deficiency of vitamin B6 or pyridoxine causes higher endogenous oxalate production and accumulation of peroxisomal glyoxalate which is oxidized to oxalate. The prevalence of hyperoxaluria is estimated at 5-24% of all patients with gastrointestinal diseases associated with malabsorption (Nephrol. Dial. Transplant. 2016, March: Lama Nazzal, et al).
The prevalence of CaOx stones is 20-30% in patients with jejunoileal bypass. The prevalence of EH is estimated at 29-74% in post-RYGB surgery patients.

